
– Published in the Lancet Global Health Volume 6, No. 6, e609–e610, June 2018
Drug prices are controversial in all countries, and nowhere more so than in low-income and middle-income countries, where access to essential drugs is very price sensitive. The higher the price, the fewer the patients who can be treated, so therefore the aim is to maintain drug prices consistently low. However, it is unclear whether the lowest price for a drug will always be the best value, and it is an issue that many purchasers must consider. Will quality be compromised? Will the bidder offering the lowest price be able to deliver on time and in full? Unsatisfactory answers to these key questions will put lives at risk.1
Since 2005, the Partnership for Supply Chain Management (PFSCM) has been providing procurement services to the US Government, the Global Fund to fight AIDS, Tuberculosis and Malaria, and other public-sector clients worldwide, supplying over 5 billion US$ in health commodities. Procurement of health commodities is complex. Some evaluation criteria used for procurement of health commodities by PFSCM are absolute. For instance, the product must be of the right quality, as indicated by pre-qualification by the WHO or approval by a stringent regulatory authority. The product must be suitable for the country in which it will be used, registered for use in that country, and have sufficient shelf life left to be used before expiry.
Two important best practices are used by PFSCM that may seem counterintuitive to non-experts but have resulted in lower drug prices and better outcomes. Purchasing from multiple competitively priced suppliers, rather than purchasing only from the supplier offering the lowest price, incentivises more suppliers to stay in the market. This practice helps drive prices down over time and reduces the likelihood of stockouts. In addition, coordinating procurement and streamlining product selection helps phase out inferior drug formulations and improves the availability of optimal drug formulations.
To procure from multiple suppliers, PFSCM begins by verifying the eligibility of offers received on the basis of donor and country requirements. The next step involves verifying product-specific eligibility criteria. Only then does PFSCM address qualitative and quantitative factors such as delivery time, past performance of vendors, remaining and total shelf life, available production capacity, current orders, and price, to make a judgement on best value. PFSCM closely considers the dynamics of the market to maintain a viable number of vendors to sustain competition.
From PFSCM’s own experience procuring health commodities, when a drug loses patent protection or is licensed for generic production, the first-to-market generic supplier sets prices at least 20% below the patent holder. A second entrant will then often set the price around 10% lower. Once the third, fourth, or fifth suppliers enter the market, competition gets fiercer, and prices drop strikingly to a level at which most procurement prices are within a 5% band.
PFSCM has developed an award matrix (see below) to distribute supply over multiple vendors, incentivising a broader supplier base. Each vendor that is considered for an award must set a price that is within the competitive range, which is usually between 2% and 5% below the lowest compliant offer. With this award matrix, PFSCM establishes a minimum order quantity per product per supplier, while ensuring that transport costs are optimised. The actual percentages awarded by PFSCM to each vendor also consider production batch size, container loading, and delivery time.
Table:

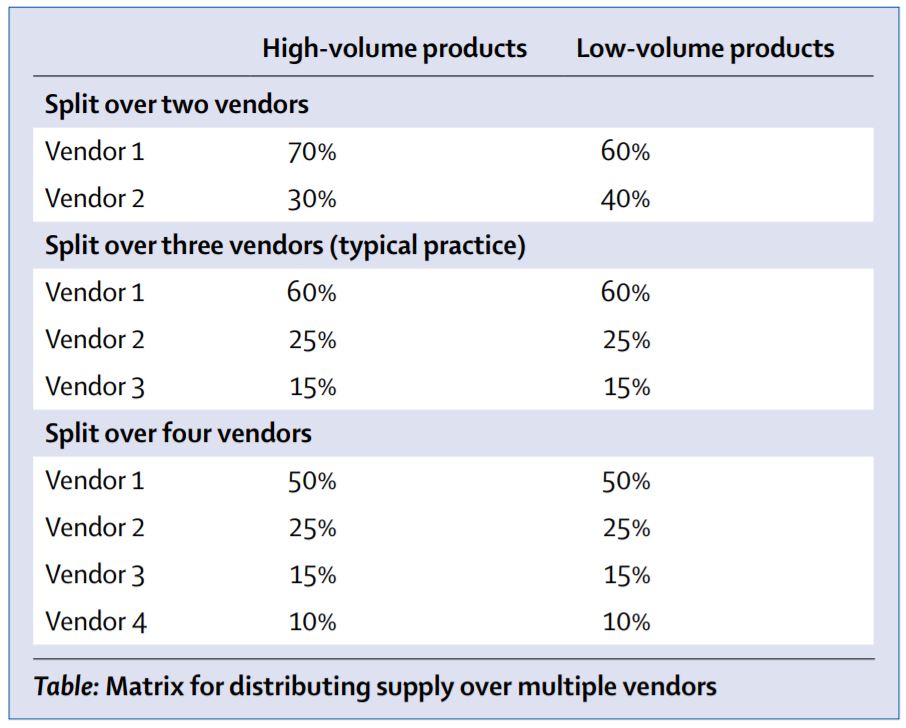
Matrix for distributing supply over multiple vendors
Although price is an important factor to consider when maximising the amount of procured health commodities, it is not the only one involved in granting a procurement award. Considering all other factors besides just the cost of the drug will lead to the timely, reliable delivery of safe, high-quality products, and ultimately result in lower prices from increased competition. This strategy ensures that lifesaving treatments are not withheld unnecessarily from the people who need them most.In addition to engaging multiple vendors to promote competition, the second important strategy that PFSCM considers involves consolidating demand and coordinating procurement in a regularly scheduled manner.
This practice demonstrates commercial viability to generic drug manufacturers, reduces lead times, and avoids stockouts.2 The ARV Procurement Working Group (APWG) follows this strategy to ensure coordinated placement of orders to avoid production delays.3 A suitable level of coordination among stakeholders helps steer the market towards optimal drug formulations, by phasing out inferior drug formulations and introducing new and more effective formulations. This ensures that clinically important, low-volume antiretrovirals are maintained in the market.2 Using a coordinated and streamlined product selection process, APWG helped increase the proportion of optimal paediatric antiretrovirals purchased from 88% to 95% between 2013 and 2015, while the mean total lead time decreased from 84 days to 63 days.2
References:
1. Tren, R, Hess, K, and Bate, R. Drug procurement, the Global Fund and misguided competition policies. Malar J. 2009; 8: 305
2. APWG. Case study: sustaining paediatric ARV supply security with the Paediatric ARV Procurement Working Group.
https://www.theglobalfund.org/media/6492/psm_paediatricarvprocurementworkinggroupcasestudy_report_en.pdf
3. The Global Fund. Sourcing and management of health products: antiretrovirals.
https://www.theglobalfund.org/en/sourcing-management/health-products/antiretrovirals/









